All content on this site is intended for healthcare professionals only. By acknowledging this message and accessing the information on this website you are confirming that you are a healthcare professional.
The PsOPsA Hub website uses a third-party service provided by Google that dynamically translates web content. Translations are machine generated, so may not be an exact or complete translation, and the PsOPsA Hub cannot guarantee the accuracy of translated content. The PsOPsA Hub and its employees will not be liable for any direct, indirect, or consequential damages (even if foreseeable) resulting from use of the Google Translate feature. For further support with Google Translate, visit Google Translate Help.


The PsOPsA Hub is an independent medical education platform. This activity is supported by an educational grant from Lilly. Funders are allowed no direct influence on our content.
Now you can support HCPs in making informed decisions for their patients
Your contribution helps us continuously deliver expertly curated content to HCPs worldwide. You will also have the opportunity to make a content suggestion for consideration and receive updates on the impact contributions are making to our content.
Find out more
Create an account to access:
Bookmark & personalize site content
Receive alerts for new content in your areas of interest
View psoriasis and psoriatic arthritis content recommended for you
Case study | diagnosing unspecific back pain in a 67-year-old patient with psoriasis and PsA
Patients with psoriasis and psoriatic arthritis (PsA) may present with unspecific back and spinal pain, which may be related to their psoriatic disease.1 Here, we summarize a case study originally presented by Vladimirova at the European Alliance of Associations for Rheumatology (EULAR) 2023 Congress.1 This case highlights the importance of imaging for the differential diagnosis of patients with psoriasis.
Figure 1. Patient history*

NSAID, non-steroidal anti-inflammatory drug.
*Data from Vladimirova.1
The patient was diagnosed with psoriasis in their early 20's.1 They developed PsA during their first pregnancy and then, during their second pregnancy, developed pelvic pain which did not resolve after delivery. During their thirties, this patient also developed cervical spine pain, nail psoriasis, and non-radiographic axial PsA. The patient timeline and treatments given are shown in Figure 2.1
Figure 2. Patient timeline, with diagnoses and treatments*

NSAID, non-steroidal anti-inflammatory drug; PsA, psoriatic arthritis, UV, ultraviolet radiation.
*Data from Vladimirova.1
After experiencing lower back and buttock pain, especially in the left hip, an MRI of sacroiliac joint revealed sacroiliitis and bilateral bone marrow oedema with T1 structural changes.1 No radiographic changes were found in the sacroiliac joint. The patient was diagnosed with non-radiographic axial PsA at age 43, and treatment was changed to an interleukin-17 inhibitor (secukinumab) to cover all affected domains.1
Hypothetically, a proposed flare of symptoms has affected the patient at age 67. The problems that the patient is experiencing are shown in Figure 3 and a treatment plan is outlined in Figure 4.
Figure 3. Patient symptoms*

CT, computed tomography; MRI, magnetic resonance imaging; NSAID, non-steroidal anti-inflammatory drug.
*Data from Vladimirova.1
Figure 4. Treatment plan*

*Data from Vladimirova.1
Degenerative vs inflammatory disease: How can imaging help?2
In this case study, imaging was informative when diagnosing the causes of back pain. Imaging can also help clinicians to identify whether psoriatic disease is degenerative or inflammatory. Figure 5 illustrates which imaging techniques can be applied to each indication, but does not take into account the specificity of each technique.
Figure 5. Effectiveness of imaging techniques*
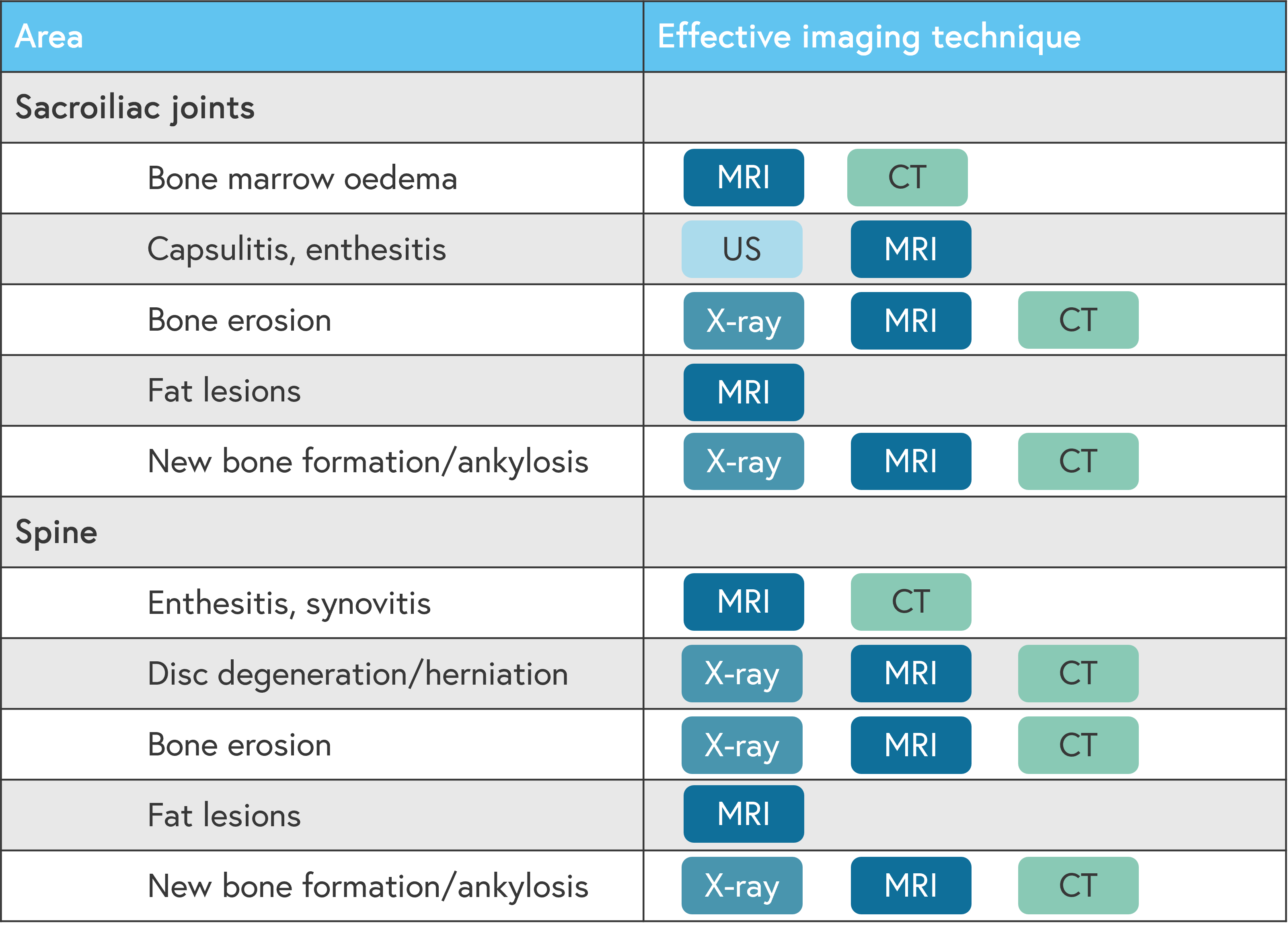
CT, computed tomography; MRI, magnetic resonance imaging; US, ultrasound.
*Adapted from Østergaard.2
References
Please indicate your level of agreement with the following statements:
The content was clear and easy to understand
The content addressed the learning objectives
The content was relevant to my practice
I will change my clinical practice as a result of this content